
Volume 12, Issue 2 (10-2024)
Jorjani Biomed J 2024, 12(2): 14-18 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abdulelah Abbas Al-Hadeethi A, Taghian F, Jawad Mohammed Al-Jawad Z, Jalali Dehkordi K. Comparative effects of high-intensity interval training and moderate-intensity interval training on CK/LDH/IL-6 markers in male goalball players with visual impairments. Jorjani Biomed J 2024; 12 (2) :14-18
URL: http://goums.ac.ir/jorjanijournal/article-1-1045-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-1045-en.html
Ahmed Abdulelah Abbas Al-Hadeethi1 

 , Farzaneh Taghian2 , Zaydoon Jawad Mohammed Al-Jawad3 , Khosro Jalali Dehkordi1
, Farzaneh Taghian2 , Zaydoon Jawad Mohammed Al-Jawad3 , Khosro Jalali Dehkordi1
, Farzaneh Taghian2 , Zaydoon Jawad Mohammed Al-Jawad3 , Khosro Jalali Dehkordi1
1- Department of Sports Physiology, Faculty of Sports Sciences, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan
2- Department of Sports Physiology, Faculty of Sports Sciences, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan ,ft.taghian@gmail.com
3- Faculty of Physical Education and Sports Sciences, University of Baghdad, Baghdad, Iraq
2- Department of Sports Physiology, Faculty of Sports Sciences, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan ,
3- Faculty of Physical Education and Sports Sciences, University of Baghdad, Baghdad, Iraq
Full-Text [PDF 554 kb]
(262 Downloads)
| Abstract (HTML) (1675 Views)
Discussion
The present research was conducted to compare and investigate the effects of HIIT and MIIT for eight weeks on the concentration of IL-6, CK, and LDH of goalball players. The present study showed that HIIT and MIIT for eight weeks caused changes in the concentration of CK, LDH, and IL-6 in the serum level of goalball athletes. The results showed a significant decrease (P-Value < 0.001) in CK, LDH, and IL-6 levels due to HIIT compared to MIIT for eight weeks in goalball players.
Several studies have examined the physiological responses of goalball athletes under various conditions, including laboratory settings, field tests, and in-game scenarios (8). Within the laboratory context, a predominant focus has been placed on investigating the morphological profiles of these athletes alongside anthropometric measurements and overall physical fitness parameters (8,15,16). This study evaluated the CK/LDH/IL-6 concentrations in two exercise protocols. We found that HIIT and MIIT for eight weeks caused changes in the concentration of CK in the serum level of goalball athletes. The results showed a significant decrease (P-Value < 0.001) in CK levels due to HIIT compared to MIIT for eight weeks in goalball players. As a result, the study found a marked decrease in CK levels in the HIIT group compared to the control group, indicating that while HIIT can initially induce muscle damage, it also promotes adaptations that enhance muscle integrity over time. Conversely, MIIT, characterized by sustained moderate exertion, typically elicits a more stable inflammatory response and less acute muscle damage than HIIT. The study demonstrated that while HIIT and MIIT reduced CK levels, the changes were more pronounced in the HIIT group. The data suggests that the higher intensity of exercise in HIIT may lead to more significant initial muscle damage, but with consistent training, athletes may develop improved recovery mechanisms that lower CK levels over time.
The significant decrease in CK and LDH levels observed in the HIIT group implies that this training modality induces muscle damage and promotes recovery adaptations over time. For goalball athletes, this means that regular HIIT sessions can improve muscle integrity and resilience, allowing players to withstand the physical demands of the sport more effectively. Additionally, reducing IL-6 levels following HIIT suggests a potential anti-inflammatory effect, which can contribute to faster recovery times and reduced risk of overuse injuries. This is particularly important in goalball, where athletes are prone to muscle fatigue and inflammation due to the sport's unique demands, including rapid sprints, abrupt changes in direction, and high anaerobic exertion. In practical terms, coaches and trainers can utilize these findings to design more effective training programs that balance intensity and recovery. By integrating HIIT into the training schedule, goalball players can enhance their aerobic and anaerobic capacities, improving their performance during matches. Furthermore, understanding the physiological responses to different training intensities allows for better monitoring of athletes' recovery needs, enabling more tailored training approaches that consider individual responses to exercise.
CK is a crucial protein involved in muscle metabolism, and its concentration is commonly recognized as a biomarker for physical stress (17). The presence of CK in the plasma indicates muscle fiber damage, as it reflects the extent of leakage from damaged muscle tissue (18). The CK concentration as a biomarker allows for assessing muscle integrity and the impact of physical exertion on muscle health, providing valuable information for evaluating recovery and adaptation following intense exercise (19). LDH is an enzyme integral to various metabolic processes, especially in converting lactate to pyruvate during anaerobic metabolism (20). Due to its significant role in these pathways, LDH is frequently employed as a biomarker for assessing tissue damage and metabolic stress in the context of exercise, both during and post-activity (21). Its levels can provide valuable insights into the body's physiological responses under stress, aiding in the evaluation of muscle function and recovery (22). Elevated concentrations of LDH following exercise can indicate the degree of muscle damage and the metabolic stress experienced during HIIT (23).
IL-6, a cytokine released by muscle cells during exercise, plays a crucial role in the immune response and inflammation, making it valuable for monitoring systemic inflammatory responses induced by the physical demands of goalball. Elevated IL-6 levels can indicate muscle stress and recovery needs following HIIT and MIIT sessions. CK, an enzyme primarily found in skeletal muscle, serves as a marker for muscle integrity; its release into the bloodstream following muscle injury allows for evaluating muscle damage caused by the rapid sprints and explosive actions typical in goalball. Elevated CK levels post-exercise can inform coaches about athletes' recovery statuses and the effectiveness of the training load. Finally, LDH is involved in energy production and reflects tissue health; it is released during tissue damage and provides insights into metabolic responses and cell breakdown following intensive physical exertion. By monitoring these biomarkers, the study aims to provide a nuanced understanding of the athletes' physiological responses to training, thus aiding in optimizing training regimens and recovery strategies in goalball players.
Several studies have reported varying responses in anti-inflammatory cytokine secretion in relation to different exercise intensities, with some indicating significant increases while others show no notable changes (24,25). This inconsistency may be attributed to the transient nature of cytokines in the bloodstream, which can sometimes evade detection (25). Furthermore, cytokines are secreted by various cells and tissues, with muscle tissue being a major contributor during exercise; thus, the levels of cytokines in circulation may not accurately reflect their concentrations in the source tissues (26). Notably, IL-6 concentrations rise more significantly than other cytokines during physical activity, which may indicate muscle damage (27). In addition to exercise intensity, factors such as the type and duration of exercise also play a crucial role in influencing plasma IL-6 levels (28). Prolonged elevation of IL-6 is linked to muscle atrophy, leading to decreased strength and muscle function and increased muscle pain. Following acute exercise, elevated IL-6 levels can stimulate the secretion of IL-10 and interleukin-1 receptor antagonists (IL-1RA), both anti-inflammatory cytokines (28). Our data indicated that the eight-week HIIT and MIIT reduced the IL-6 concentration. In addition, HIIT training significantly reduced the IL-6 concentration compared with the MIIT.
Conversely, MIIT incorporates intervals of moderate exercise, enabling participants to sustain moderate exertion throughout the workout (29). This approach typically elicits a more stable inflammatory marker response than HIIT (30). Evidence suggests that MIIT may be more effective in reducing overall systemic inflammation and resulting in less muscle damage, making it a viable alternative for individuals who may find high-intensity workouts challenging (17,31). Furthermore, limited research involving individuals with moderate to high concentrations of inflammatory markers suggests that aerobic HIIT improved inflammatory markers' circulating levels (32). However, no studies have directly compared the effects of HIIT and MIIT on inflammatory cytokines and muscle damage in goalball players. Additionally, there is a lack of precise data regarding the impact of HIIT on serum levels of IL-6, CK, and LDH in goalball players (33).
In contrast with the previous study, we found that HIIT and MIIT for eight weeks could decline the IL-6 concentrations. This data might be the reason for the adaptation and hours following the final session (end of the eighth week). Research by Costello et al. (2018) and Rocha1 et al. (2017) has demonstrated significant increases in C-reactive protein (CRP), cortisol, and IL-6 following intense exercise training in trained individuals (19,34). Additionally, Dorneles et al. (2016) found that intense intermittent exercise led to increased levels of LDH and CK, suggesting that these inflammatory and muscle-damage markers can rise after strenuous exercise. The study which examining muscle damage indicators, such as CK and LDH, has shown elevations persisting for up to 24 to 48 hours post-exercise (35). Acute increases in LDH levels are anticipated following HIIT sessions due to the stress and damage experienced by muscle tissue. However, with consistent training, adaptations can occur that enhance the muscle's capacity to manage oxidative stress, which may result in reduced LDH responses in subsequent workouts. This increase in LDH levels is a marker for the physiological impact of vigorous exercise, reflecting the extent of muscular trauma and the body's subsequent stress response (36). Monitoring LDH levels can provide essential insights into recovery needs and the overall effects of intense physical activity on muscle health (37).
CK results were very discrepant, as half of the studies showed no alterations immediately after intense or moderate exercise, while the other half showed increased CK levels (38). Moghadam Kia et al. (2016) stated that CK levels significantly vary according to sex and race (38). The degree of this change depended on the duration and type of exercise, with strenuous exercise being responsible for greater elevations (38). Damaged muscle fiber structures were pointed out as being the cause for the rise, but one study of repeated eccentric exercise caused almost no increase in CK levels (39). CK levels demonstrate considerable variability influenced by factors such as sex, race, and the type of exercise performed. Notably, eccentric exercise is generally associated with more significant muscle damage compared to concentric contractions of the same intensity. This discrepancy highlights the importance of considering these variables when interpreting CK levels as muscle stress and damage indicators (40). Understanding these differences is essential for accurately assessing muscle response and recovery in diverse populations and exercise modalities (41).
Consequently, delayed onset muscle soreness and associated inflammatory responses are typically observed within this time. Pal et al. (2018) also noted that interval training increases LDH, CK, and liver enzyme levels within 24 to 48 hours following training. Therefore, the timing of assessments after HIIT is critical for evaluating inflammation and muscle damage markers (42). Given that individuals with overweight status often exhibit lower physical fitness levels, it is essential to consider the effects of high-intensity training, particularly HIIT (43). Rohnejad and colleagues investigated the acute effects of HIIT on inflammatory and muscle damage indices in overweight middle-aged men and the kinetics of these markers at 1, 24, and 48 hours post-training (44). Additionally, these markers correlate with frailty, morbidity, and mortality. Notably, CRP levels are lower in individuals who engage in moderate exercise than those who are inactive (32,45).
The majority of studies have reported an increase in IL-10 following intense exercise, aligning with earlier findings (32,46). However, Allen et al. (2017) highlighted that IL-10 production in response to strenuous acute exercise is variable, with some studies reporting increases, others indicating decreases, and some showing no changes, depending on the exercise protocols and analytical methods employed (32). Nonetheless, IL-10 levels typically peak during the recovery phase post-exercise, with the extent of this increase being associated with both the active muscle mass engaged and the intensity of the exercise performed. Recent reviews by Cabral‐Santos et al. (2019) emphasize that the duration of training is the most critical factor influencing the magnitude of the exercise-induced increase in plasma IL-10 levels (47). This elevation in IL-10 may protect against potential chronic low-grade inflammation and tissue damage.
In a competitive tournament setting, goalball athletes may be required to participate in multiple matches within a condensed timeframe. Assessing the concentrations of IL-6, CK, and LDH 48 hours post-training can provide valuable insights into the recovery processes of players between games, as well as the potential impact on their performance in subsequent competitions. Furthermore, an elevation in IL-6, CK, and LDH levels following exercise can indicate muscle damage or fatigue, heightening the risk of injury. By closely monitoring these biomarker concentrations, coaches can effectively identify players who may be predisposed to injury and implement appropriate preventive strategies.
It is essential to consider that the participants in this study are individuals with special needs, and the act of venipuncture can elicit discomfort and sensitivity. Consequently, the optimal approach would involve conducting blood sampling 48 hours after the exercise sessions. Additionally, it is recommended to evaluate biomarker levels immediately post-training and at 6, 12, and 24 hours after that. These considerations are acknowledged as limitations within the scope of the study. One of the limitations of the present study is the lack of control over the psychological conditions of the players. The following limitation was that the current study was conducted on male goalball players aged 21 to 27 years, and the generalization of the results is only possible on similar age and gender groups. Another limitation of this study is the lack of measuring variables immediately, 12 hours, and 24 hours after the exercises. Due to the fact that the test subjects were particular (Blind or severely visually impaired) and were sensitive to blood sampling and invasive methods, we were faced with this limitation. It is better to investigate the effect of such exercises on other age and gender groups in future research due to the limitations of the current research. Moreover, the functional tests of this sport should be evaluated, and their relationship with physiological changes in the players should be investigated and analyzed. Also, by conducting a similar study in different sports and comparing its results with the present study, a practical solution can be provided to improve players' performance, reduce the risk factors of injury, and prevent them.
In summary, the changes in IL-6, CK, and LDH levels observed in the study reflect the physiological responses to different training intensities. While initially causing more significant muscle damage and metabolic stress, HIIT fosters adaptations that improve muscle recovery and integrity, as evidenced by the substantial reductions in CK and LDH levels over the training period. In contrast, MIIT promotes a more stable response with less acute damage, highlighting the importance of training intensity in influencing muscle health and recovery in goalball players.
Conclusion
Our study demonstrated that HIIT and MIIT for eight weeks could improve the concentration of CK, LDH, and IL-6 in goalball players. Moreover, HIIT had more effect than MIIT for eight weeks. Based on our data, performing HIIT and MIIT may consistently increase the capacity of the physiology of goalball players.
Acknowledgement
No acknowledgment.
Funding sources
No funding.
Ethical statement
All procedures have been approved by the ethics committee of Islamic Azad University of Isfahan (Khorasgan) with the number IR.IAU.KHUISF.REC.1402.381 and were carried out according to the Declaration of Helsinki. Before starting the study, informed consent was obtained from all the participants who participated in the study.
Conflicts of interest
The authors declare that they have no conflict of interest.
Author contributions
AM carried out the experiments and drafted the manuscript, FT participated in this study as supervisor and contributed to study design, conceptualization, data analysis and validation, and revising the manuscript. KhJD and ZJ participated in data validation and revising the manuscript. All authors read and approved the final manuscript.
Full-Text: (108 Views)
Introduction
Goalball is a Paralympic sport designed for individuals with visual impairments (1). Most research on goalball players has focused on functional, anthropometric, and morphological evaluations (1,2). However, the potential correlations between physiological fitness and responses observed during the game and technical performance remain underexplored in the existing literature (3,4).
Interval training (IT) has emerged as a time-efficient alternative to traditional training programs, particularly in managing physiological performance (5). High-intensity interval Training (HIIT) represents a specific form of interval training that alternates short bursts of high-intensity anaerobic exercise with periods of lower-intensity recovery (5,6). Studies have indicated that goalball players are particularly susceptible to inflammation and muscle damage due to the unique physical demands of the sport, which combines HIIT actions with anaerobic energy systems. The game involves rapid sprints, abrupt changes in direction, and explosive movements, all of which require significant muscular exertion and can lead to microtrauma in muscle fibers. During gameplay, athletes often reach heart rates between 85% and 100% of their maximal capacity, primarily relying on anaerobic metabolism, which can result in the accumulation of metabolic byproducts. This high-intensity effort is associated with acute increases in inflammatory markers, including interleukin-6 (IL-6), as the body responds to muscle damage and stress (7-9).
Moreover, the nature of goalball training, which often incorporates HIIT and moderate-intensity interval training (MIIT), further exacerbates the potential for inflammation and muscle damage. In this regard, HIIT, characterized by short bursts of maximal effort followed by recovery periods, can lead to significant physiological stress and subsequent inflammatory responses. While HIIT effectively improves cardiovascular fitness and muscle strength, it can also induce acute elevations in muscle damage markers such as creatine kinase (CK) and lactate dehydrogenase (LDH) immediately following training sessions. Exercise training significantly strains muscles, leading to high lactate accumulation and delayed onset muscle soreness (DOMS) (10,11). Research conducted on athletes in wheelchair basketball has shown significant elevations in inflammatory markers, such as IL-6 and tumor necrosis factor-alpha (TNF-α), following intense competition, indicating a robust inflammatory response similar to that observed in goalball players (12). Additionally, a study on para-athletes participating in track and field events reported increased levels of CK and LDH post-competition, suggesting that the physical demands of these sports lead to muscle damage comparable to that experienced in goalball (13).
Furthermore, investigations into the effects of HIIT in athletes with disabilities, such as those competing in sitting volleyball, have demonstrated that HIIT can effectively modulate inflammatory responses and muscle damage markers, paralleling the current study's findings (14). These studies collectively highlight the importance of understanding how different forms of exercise impact inflammatory and muscle damage markers across various sports, particularly those with similar anaerobic demands. These findings provide further context for the current study, reinforcing that HIIT, as employed in goalball, can lead to measurable changes in muscle damage and inflammatory markers (12).
In this study, IL-6, CK, and LDH were selected as biomarkers due to their significant roles in assessing physiological responses to exercise, particularly in the context of goalball training. Consequently, the current study aimed to compare the relationships between physiological parameters measured in controlled laboratory environments and those recorded during simulated game scenarios. Furthermore, this research aimed to explore the correlations between these physiological metrics and technical performance outcomes in goalball. By establishing these connections, this study aimed to understand better how physiological factors influence performance in competitive settings.
Methods
Participants
Twenty-four male elite goalball players from the Isfahan City Team participated in this study (Age 20-34 years, weight 78-98 kg, height 172-188 cm, experience level in goalball 4-12 years). The athletes were categorized into three groups according to the exercise training intensity.
To determine the sample size, the sample size estimation software (G*POWER) was used, considering the significance level of 0.05, the effect size of 0.4, and the test power of 0.8. Based on the analysis of this software, the number of 24 people was determined. Subjects were selected purposefully and available and were randomly assigned to three homogenous groups, including high-intensity exercises (HIIT, eight people), moderate-intensity exercises (MIIT, eight people), and a control group (Eight people).
Their training program was based on three sessions a week for two months. The inclusion criteria were having at least five years of playing experience, absence of medical restrictions (Illness and injury), history of surgery, and willingness to participate. The exclusion criteria were an injury in the last 30 days, or a history of surgery that would limit their attendance. It should be noted that the control group's activity level was monitored. Moreover, the control group was explicitly instructed to maintain their usual lifestyle activities and refrain from structured physical exercise.
Furthermore, participants' self-reports were utilized to confirm adherence to their routine. Participants' self-reports are essential to establish a baseline for comparison with the exercise intervention groups. In addition, emphasis has been placed on the control group's importance in evaluating the intervention groups' physiological and performance outcomes. To control the intensity of the exercises in the training, the subject's heart rate was monitored before and after each session by the researcher using a heart rate monitor device (Beurer FT-90, made in Germany). The following formula was used to calculate the reserve heart rate percentage.
Percentage of reserve heart rate = Maximum heart rate - resting heart rate
Exercise protocol
During the initial sessions, the instructor engaged the participants in a discussion regarding the class schedule, exercise execution, and the specific characteristics of each exercise. The instructor also inquired about any feelings of fatigue or incapacity the participants may have experienced and any challenges encountered during or between training sessions. Issues were raised with both the trainer and the researcher to ensure a supportive training environment. Following this introductory conversation, lasting approximately 15 minutes, participants commenced the prescribed exercises under the trainer's supervision.
The HIIT program comprised a structured warm-up phase lasting 15 minutes, which began with low-intensity jogging at 50% of the heart rate reserve (HRR). This was followed by three sets of intermittent running, consisting of 30 seconds of fast jogging, followed by 30 seconds of slow jogging, and concluded with 5 minutes of dynamic stretching. Throughout the 8-week HIIT training program, participants engaged in 30-second intervals of running at intensities starting at 100% of their HRR during the first and second weeks and gradually increasing to 200% of their HRR by the seventh and eighth weeks. The active recovery period was set at 30 seconds, during which participants jogged at 50% of their HRR for a total of four sets, with 5 minutes of passive recovery implemented between rounds (Table 1) (14-16).
Goalball is a Paralympic sport designed for individuals with visual impairments (1). Most research on goalball players has focused on functional, anthropometric, and morphological evaluations (1,2). However, the potential correlations between physiological fitness and responses observed during the game and technical performance remain underexplored in the existing literature (3,4).
Interval training (IT) has emerged as a time-efficient alternative to traditional training programs, particularly in managing physiological performance (5). High-intensity interval Training (HIIT) represents a specific form of interval training that alternates short bursts of high-intensity anaerobic exercise with periods of lower-intensity recovery (5,6). Studies have indicated that goalball players are particularly susceptible to inflammation and muscle damage due to the unique physical demands of the sport, which combines HIIT actions with anaerobic energy systems. The game involves rapid sprints, abrupt changes in direction, and explosive movements, all of which require significant muscular exertion and can lead to microtrauma in muscle fibers. During gameplay, athletes often reach heart rates between 85% and 100% of their maximal capacity, primarily relying on anaerobic metabolism, which can result in the accumulation of metabolic byproducts. This high-intensity effort is associated with acute increases in inflammatory markers, including interleukin-6 (IL-6), as the body responds to muscle damage and stress (7-9).
Moreover, the nature of goalball training, which often incorporates HIIT and moderate-intensity interval training (MIIT), further exacerbates the potential for inflammation and muscle damage. In this regard, HIIT, characterized by short bursts of maximal effort followed by recovery periods, can lead to significant physiological stress and subsequent inflammatory responses. While HIIT effectively improves cardiovascular fitness and muscle strength, it can also induce acute elevations in muscle damage markers such as creatine kinase (CK) and lactate dehydrogenase (LDH) immediately following training sessions. Exercise training significantly strains muscles, leading to high lactate accumulation and delayed onset muscle soreness (DOMS) (10,11). Research conducted on athletes in wheelchair basketball has shown significant elevations in inflammatory markers, such as IL-6 and tumor necrosis factor-alpha (TNF-α), following intense competition, indicating a robust inflammatory response similar to that observed in goalball players (12). Additionally, a study on para-athletes participating in track and field events reported increased levels of CK and LDH post-competition, suggesting that the physical demands of these sports lead to muscle damage comparable to that experienced in goalball (13).
Furthermore, investigations into the effects of HIIT in athletes with disabilities, such as those competing in sitting volleyball, have demonstrated that HIIT can effectively modulate inflammatory responses and muscle damage markers, paralleling the current study's findings (14). These studies collectively highlight the importance of understanding how different forms of exercise impact inflammatory and muscle damage markers across various sports, particularly those with similar anaerobic demands. These findings provide further context for the current study, reinforcing that HIIT, as employed in goalball, can lead to measurable changes in muscle damage and inflammatory markers (12).
In this study, IL-6, CK, and LDH were selected as biomarkers due to their significant roles in assessing physiological responses to exercise, particularly in the context of goalball training. Consequently, the current study aimed to compare the relationships between physiological parameters measured in controlled laboratory environments and those recorded during simulated game scenarios. Furthermore, this research aimed to explore the correlations between these physiological metrics and technical performance outcomes in goalball. By establishing these connections, this study aimed to understand better how physiological factors influence performance in competitive settings.
Methods
Participants
Twenty-four male elite goalball players from the Isfahan City Team participated in this study (Age 20-34 years, weight 78-98 kg, height 172-188 cm, experience level in goalball 4-12 years). The athletes were categorized into three groups according to the exercise training intensity.
To determine the sample size, the sample size estimation software (G*POWER) was used, considering the significance level of 0.05, the effect size of 0.4, and the test power of 0.8. Based on the analysis of this software, the number of 24 people was determined. Subjects were selected purposefully and available and were randomly assigned to three homogenous groups, including high-intensity exercises (HIIT, eight people), moderate-intensity exercises (MIIT, eight people), and a control group (Eight people).
Their training program was based on three sessions a week for two months. The inclusion criteria were having at least five years of playing experience, absence of medical restrictions (Illness and injury), history of surgery, and willingness to participate. The exclusion criteria were an injury in the last 30 days, or a history of surgery that would limit their attendance. It should be noted that the control group's activity level was monitored. Moreover, the control group was explicitly instructed to maintain their usual lifestyle activities and refrain from structured physical exercise.
Furthermore, participants' self-reports were utilized to confirm adherence to their routine. Participants' self-reports are essential to establish a baseline for comparison with the exercise intervention groups. In addition, emphasis has been placed on the control group's importance in evaluating the intervention groups' physiological and performance outcomes. To control the intensity of the exercises in the training, the subject's heart rate was monitored before and after each session by the researcher using a heart rate monitor device (Beurer FT-90, made in Germany). The following formula was used to calculate the reserve heart rate percentage.
Percentage of reserve heart rate = Maximum heart rate - resting heart rate
Exercise protocol
During the initial sessions, the instructor engaged the participants in a discussion regarding the class schedule, exercise execution, and the specific characteristics of each exercise. The instructor also inquired about any feelings of fatigue or incapacity the participants may have experienced and any challenges encountered during or between training sessions. Issues were raised with both the trainer and the researcher to ensure a supportive training environment. Following this introductory conversation, lasting approximately 15 minutes, participants commenced the prescribed exercises under the trainer's supervision.
The HIIT program comprised a structured warm-up phase lasting 15 minutes, which began with low-intensity jogging at 50% of the heart rate reserve (HRR). This was followed by three sets of intermittent running, consisting of 30 seconds of fast jogging, followed by 30 seconds of slow jogging, and concluded with 5 minutes of dynamic stretching. Throughout the 8-week HIIT training program, participants engaged in 30-second intervals of running at intensities starting at 100% of their HRR during the first and second weeks and gradually increasing to 200% of their HRR by the seventh and eighth weeks. The active recovery period was set at 30 seconds, during which participants jogged at 50% of their HRR for a total of four sets, with 5 minutes of passive recovery implemented between rounds (Table 1) (14-16).
.PNG)
The MIIT (MIIT) program included continuous running at a moderate intensity. In the first week, participants ran for 25 minutes at an intensity corresponding to 40-50% of their HRR. During the second week, the duration remained the same, but the intensity was increased to 50-55% of the HRR. From the third to the seventh week, the participants ran for 30 minutes at an intensity of 55-60% of their HRR. Finally, in the eighth week, the training session consisted of running for 30 to 35 minutes at an intensity of 60-65% of the HRR. This gradual progression in both duration and intensity aimed to enhance aerobic fitness and improve overall endurance in the participants (Table 2) (14-16). The control group was instructed to maintain regular daily routines without engaging in structured physical exercise. This allowed researchers to observe the effects of the exercise interventions by comparing physiological and performance parameter changes between the exercise groups and those who did not participate in any increased physical activity. The control group's adherence to their usual lifestyle served as a baseline reference for evaluating the impact of the HIIT and MIIT programs on the participants in the experimental groups.
.PNG)
Blood collection and sampling
To assess biochemical variables, 5 ml of blood was collected from the athletes both before and after the training interventions. Venous blood was drawn from the brachial vein of the left arm after a fasting period of 12 hours, specifically 24 hours prior to the first training session and 24 hours following the final session (End of the eighth week). Collections occurred between 8 to 10 AM and were conducted using tubes containing the anticoagulant EDTA.
Following collection, the blood samples were immediately centrifuged at a speed of 2,000 to 3,000 RPM for 10 minutes using a centrifuge manufactured by Eppendorf. The centrifugation speed was measured using relative centrifugal force (RCF). The resulting serum was frozen at -80 °C until testing.
Blood samples were transported to the laboratory while adhering to safety protocols and maintaining cold temperature chains to ensure sample integrity. The levels of IL-6 were measured using a kit from Elabsciense (E-EL-H6156), which has a sensitivity of 0.94 pg/mL and a detection range of 1.56-100 pg/mL. Additionally, enzymatic kits from Delta Darman in Iran were utilized to measure levels of CK and LDH before and after the training interventions.
Statistical analysis
After data collection, SPSS version 27 software was used for statistical data analysis. Furthermore, the repeated measures ANOVA test was used to examine the changes in the indicators studied. The Post hoc Bonferroni test was used for pairwise comparisons. The model's basic assumptions, such as the error distribution's normality, the error variance's homogeneity, and the variance-covariance matrix's homogeneity, were examined and confirmed by the Shapiro-Wilk and Levene's tests, respectively. Repeated measures ANOVA test was used to compare the individual characteristics of the subjects of the two groups and consider the assumption of normality of the data in each group. The results' descriptive statistics level is mean±standard deviation (SD). The significance level was set at P-Value < 0.05 in all analyses.
Results
The muscle damage markers were changed by HIIT and MITT protocols
The results revealed that after eight weeks of HIIT and MIIT, there was a significant difference in the concentrations of CK (Figure 1a, P-Value <0.001) and LDH (Figure 1b, P-Value > 0.001). Also, the concentration of the CK and LDH significantly reduced in the HIIT (Figure 1a, P-Value < 0.001) and MIIT (Figure 1b, P-Value > 0.001) groups compared with the control group. As a result, the study found a marked decrease in CK levels in the HIIT group compared to the control group, indicating that while HIIT could initially induce muscle damage, it also promoted adaptations that enhance muscle integrity over time (Figure 1a, P-Value < 0.001). Conversely, MIIT, characterized by sustained moderate exertion, typically elicited a more stable inflammatory response and less acute muscle damage compared to HIIT (Figure 1a, P-Value < 0.001). The study demonstrated that while HIIT and MIIT reduced CK levels, the changes were more pronounced in the HIIT group (Figure 1a, P-Value < 0.001), suggesting that the higher intensity of exercise in HIIT might lead to more significant initial muscle damage; however, with consistent training, athletes may develop improved recovery mechanisms that lower CK levels over time.
Similarly, LDH is a marker for metabolic stress and tissue damage, particularly during anaerobic metabolism. The study indicated that LDH levels also decreased significantly in both training groups compared to the control group, with HIIT showing a more substantial reduction (Figure 1b, P-Value > 0.001). This aligns with the understanding that HIIT, while inducing acute increases in LDH due to the high metabolic demands, ultimately leads to adaptations that enhance the muscle's ability to manage oxidative stress and recover from intense exercise (Figure 1b, P-Value > 0.001). Our findings indicated that performing HIIT decreased the CK (Figure 1a, P-Value < 0.001) and LDH (Figure 1b, P-Value < 0.023) concentrations compared to the MIIT.
To assess biochemical variables, 5 ml of blood was collected from the athletes both before and after the training interventions. Venous blood was drawn from the brachial vein of the left arm after a fasting period of 12 hours, specifically 24 hours prior to the first training session and 24 hours following the final session (End of the eighth week). Collections occurred between 8 to 10 AM and were conducted using tubes containing the anticoagulant EDTA.
Following collection, the blood samples were immediately centrifuged at a speed of 2,000 to 3,000 RPM for 10 minutes using a centrifuge manufactured by Eppendorf. The centrifugation speed was measured using relative centrifugal force (RCF). The resulting serum was frozen at -80 °C until testing.
Blood samples were transported to the laboratory while adhering to safety protocols and maintaining cold temperature chains to ensure sample integrity. The levels of IL-6 were measured using a kit from Elabsciense (E-EL-H6156), which has a sensitivity of 0.94 pg/mL and a detection range of 1.56-100 pg/mL. Additionally, enzymatic kits from Delta Darman in Iran were utilized to measure levels of CK and LDH before and after the training interventions.
Statistical analysis
After data collection, SPSS version 27 software was used for statistical data analysis. Furthermore, the repeated measures ANOVA test was used to examine the changes in the indicators studied. The Post hoc Bonferroni test was used for pairwise comparisons. The model's basic assumptions, such as the error distribution's normality, the error variance's homogeneity, and the variance-covariance matrix's homogeneity, were examined and confirmed by the Shapiro-Wilk and Levene's tests, respectively. Repeated measures ANOVA test was used to compare the individual characteristics of the subjects of the two groups and consider the assumption of normality of the data in each group. The results' descriptive statistics level is mean±standard deviation (SD). The significance level was set at P-Value < 0.05 in all analyses.
Results
The muscle damage markers were changed by HIIT and MITT protocols
The results revealed that after eight weeks of HIIT and MIIT, there was a significant difference in the concentrations of CK (Figure 1a, P-Value <0.001) and LDH (Figure 1b, P-Value > 0.001). Also, the concentration of the CK and LDH significantly reduced in the HIIT (Figure 1a, P-Value < 0.001) and MIIT (Figure 1b, P-Value > 0.001) groups compared with the control group. As a result, the study found a marked decrease in CK levels in the HIIT group compared to the control group, indicating that while HIIT could initially induce muscle damage, it also promoted adaptations that enhance muscle integrity over time (Figure 1a, P-Value < 0.001). Conversely, MIIT, characterized by sustained moderate exertion, typically elicited a more stable inflammatory response and less acute muscle damage compared to HIIT (Figure 1a, P-Value < 0.001). The study demonstrated that while HIIT and MIIT reduced CK levels, the changes were more pronounced in the HIIT group (Figure 1a, P-Value < 0.001), suggesting that the higher intensity of exercise in HIIT might lead to more significant initial muscle damage; however, with consistent training, athletes may develop improved recovery mechanisms that lower CK levels over time.
Similarly, LDH is a marker for metabolic stress and tissue damage, particularly during anaerobic metabolism. The study indicated that LDH levels also decreased significantly in both training groups compared to the control group, with HIIT showing a more substantial reduction (Figure 1b, P-Value > 0.001). This aligns with the understanding that HIIT, while inducing acute increases in LDH due to the high metabolic demands, ultimately leads to adaptations that enhance the muscle's ability to manage oxidative stress and recover from intense exercise (Figure 1b, P-Value > 0.001). Our findings indicated that performing HIIT decreased the CK (Figure 1a, P-Value < 0.001) and LDH (Figure 1b, P-Value < 0.023) concentrations compared to the MIIT.
.PNG) Figure 1. Alternation of CK and LDH concentrations in HIIT and MIIT groups before and after eight weeks in goalball players. **Indicates a significant difference before and after the intervention in each group, a: Indicates a significant difference between the HIIT and the control groups, b: Indicates a significant difference between the MIIT and HIIT groups. |
The inflammatory marker was ameliorated by HIIT and MITT protocols
The serum concentration of IL-6 declined after performing HIIT (P-Value < 0.05) and MIIT (P-Value < 0.05) compared to before treatment (Figure 2). Notably, subjects who performed HIIT reduced the concentrations of IL-6 compared with the MIIT (Figure 2, P-Value <0.001). Therefore, HIIT might facilitate the serum concentrations of IL-6 and had anti-inflammatory activity (Figure 2, P-Value < 0.001).
The serum concentration of IL-6 declined after performing HIIT (P-Value < 0.05) and MIIT (P-Value < 0.05) compared to before treatment (Figure 2). Notably, subjects who performed HIIT reduced the concentrations of IL-6 compared with the MIIT (Figure 2, P-Value <0.001). Therefore, HIIT might facilitate the serum concentrations of IL-6 and had anti-inflammatory activity (Figure 2, P-Value < 0.001).
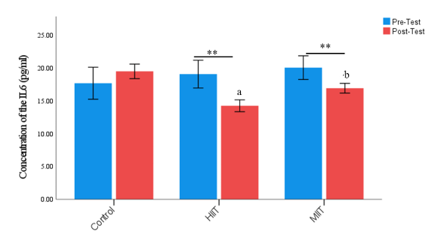 Figure 2. IL-6 concentrations in HIIT and MIIT groups before and after eight weeks in goalball players. **Indicates a significant difference before and after the intervention in each group, a: Indicates a significant difference between the HIIT and the control groups, b: Indicates a significant difference between the MIIT and HIIT groups. |
Discussion
The present research was conducted to compare and investigate the effects of HIIT and MIIT for eight weeks on the concentration of IL-6, CK, and LDH of goalball players. The present study showed that HIIT and MIIT for eight weeks caused changes in the concentration of CK, LDH, and IL-6 in the serum level of goalball athletes. The results showed a significant decrease (P-Value < 0.001) in CK, LDH, and IL-6 levels due to HIIT compared to MIIT for eight weeks in goalball players.
Several studies have examined the physiological responses of goalball athletes under various conditions, including laboratory settings, field tests, and in-game scenarios (8). Within the laboratory context, a predominant focus has been placed on investigating the morphological profiles of these athletes alongside anthropometric measurements and overall physical fitness parameters (8,15,16). This study evaluated the CK/LDH/IL-6 concentrations in two exercise protocols. We found that HIIT and MIIT for eight weeks caused changes in the concentration of CK in the serum level of goalball athletes. The results showed a significant decrease (P-Value < 0.001) in CK levels due to HIIT compared to MIIT for eight weeks in goalball players. As a result, the study found a marked decrease in CK levels in the HIIT group compared to the control group, indicating that while HIIT can initially induce muscle damage, it also promotes adaptations that enhance muscle integrity over time. Conversely, MIIT, characterized by sustained moderate exertion, typically elicits a more stable inflammatory response and less acute muscle damage than HIIT. The study demonstrated that while HIIT and MIIT reduced CK levels, the changes were more pronounced in the HIIT group. The data suggests that the higher intensity of exercise in HIIT may lead to more significant initial muscle damage, but with consistent training, athletes may develop improved recovery mechanisms that lower CK levels over time.
The significant decrease in CK and LDH levels observed in the HIIT group implies that this training modality induces muscle damage and promotes recovery adaptations over time. For goalball athletes, this means that regular HIIT sessions can improve muscle integrity and resilience, allowing players to withstand the physical demands of the sport more effectively. Additionally, reducing IL-6 levels following HIIT suggests a potential anti-inflammatory effect, which can contribute to faster recovery times and reduced risk of overuse injuries. This is particularly important in goalball, where athletes are prone to muscle fatigue and inflammation due to the sport's unique demands, including rapid sprints, abrupt changes in direction, and high anaerobic exertion. In practical terms, coaches and trainers can utilize these findings to design more effective training programs that balance intensity and recovery. By integrating HIIT into the training schedule, goalball players can enhance their aerobic and anaerobic capacities, improving their performance during matches. Furthermore, understanding the physiological responses to different training intensities allows for better monitoring of athletes' recovery needs, enabling more tailored training approaches that consider individual responses to exercise.
CK is a crucial protein involved in muscle metabolism, and its concentration is commonly recognized as a biomarker for physical stress (17). The presence of CK in the plasma indicates muscle fiber damage, as it reflects the extent of leakage from damaged muscle tissue (18). The CK concentration as a biomarker allows for assessing muscle integrity and the impact of physical exertion on muscle health, providing valuable information for evaluating recovery and adaptation following intense exercise (19). LDH is an enzyme integral to various metabolic processes, especially in converting lactate to pyruvate during anaerobic metabolism (20). Due to its significant role in these pathways, LDH is frequently employed as a biomarker for assessing tissue damage and metabolic stress in the context of exercise, both during and post-activity (21). Its levels can provide valuable insights into the body's physiological responses under stress, aiding in the evaluation of muscle function and recovery (22). Elevated concentrations of LDH following exercise can indicate the degree of muscle damage and the metabolic stress experienced during HIIT (23).
IL-6, a cytokine released by muscle cells during exercise, plays a crucial role in the immune response and inflammation, making it valuable for monitoring systemic inflammatory responses induced by the physical demands of goalball. Elevated IL-6 levels can indicate muscle stress and recovery needs following HIIT and MIIT sessions. CK, an enzyme primarily found in skeletal muscle, serves as a marker for muscle integrity; its release into the bloodstream following muscle injury allows for evaluating muscle damage caused by the rapid sprints and explosive actions typical in goalball. Elevated CK levels post-exercise can inform coaches about athletes' recovery statuses and the effectiveness of the training load. Finally, LDH is involved in energy production and reflects tissue health; it is released during tissue damage and provides insights into metabolic responses and cell breakdown following intensive physical exertion. By monitoring these biomarkers, the study aims to provide a nuanced understanding of the athletes' physiological responses to training, thus aiding in optimizing training regimens and recovery strategies in goalball players.
Several studies have reported varying responses in anti-inflammatory cytokine secretion in relation to different exercise intensities, with some indicating significant increases while others show no notable changes (24,25). This inconsistency may be attributed to the transient nature of cytokines in the bloodstream, which can sometimes evade detection (25). Furthermore, cytokines are secreted by various cells and tissues, with muscle tissue being a major contributor during exercise; thus, the levels of cytokines in circulation may not accurately reflect their concentrations in the source tissues (26). Notably, IL-6 concentrations rise more significantly than other cytokines during physical activity, which may indicate muscle damage (27). In addition to exercise intensity, factors such as the type and duration of exercise also play a crucial role in influencing plasma IL-6 levels (28). Prolonged elevation of IL-6 is linked to muscle atrophy, leading to decreased strength and muscle function and increased muscle pain. Following acute exercise, elevated IL-6 levels can stimulate the secretion of IL-10 and interleukin-1 receptor antagonists (IL-1RA), both anti-inflammatory cytokines (28). Our data indicated that the eight-week HIIT and MIIT reduced the IL-6 concentration. In addition, HIIT training significantly reduced the IL-6 concentration compared with the MIIT.
Conversely, MIIT incorporates intervals of moderate exercise, enabling participants to sustain moderate exertion throughout the workout (29). This approach typically elicits a more stable inflammatory marker response than HIIT (30). Evidence suggests that MIIT may be more effective in reducing overall systemic inflammation and resulting in less muscle damage, making it a viable alternative for individuals who may find high-intensity workouts challenging (17,31). Furthermore, limited research involving individuals with moderate to high concentrations of inflammatory markers suggests that aerobic HIIT improved inflammatory markers' circulating levels (32). However, no studies have directly compared the effects of HIIT and MIIT on inflammatory cytokines and muscle damage in goalball players. Additionally, there is a lack of precise data regarding the impact of HIIT on serum levels of IL-6, CK, and LDH in goalball players (33).
In contrast with the previous study, we found that HIIT and MIIT for eight weeks could decline the IL-6 concentrations. This data might be the reason for the adaptation and hours following the final session (end of the eighth week). Research by Costello et al. (2018) and Rocha1 et al. (2017) has demonstrated significant increases in C-reactive protein (CRP), cortisol, and IL-6 following intense exercise training in trained individuals (19,34). Additionally, Dorneles et al. (2016) found that intense intermittent exercise led to increased levels of LDH and CK, suggesting that these inflammatory and muscle-damage markers can rise after strenuous exercise. The study which examining muscle damage indicators, such as CK and LDH, has shown elevations persisting for up to 24 to 48 hours post-exercise (35). Acute increases in LDH levels are anticipated following HIIT sessions due to the stress and damage experienced by muscle tissue. However, with consistent training, adaptations can occur that enhance the muscle's capacity to manage oxidative stress, which may result in reduced LDH responses in subsequent workouts. This increase in LDH levels is a marker for the physiological impact of vigorous exercise, reflecting the extent of muscular trauma and the body's subsequent stress response (36). Monitoring LDH levels can provide essential insights into recovery needs and the overall effects of intense physical activity on muscle health (37).
CK results were very discrepant, as half of the studies showed no alterations immediately after intense or moderate exercise, while the other half showed increased CK levels (38). Moghadam Kia et al. (2016) stated that CK levels significantly vary according to sex and race (38). The degree of this change depended on the duration and type of exercise, with strenuous exercise being responsible for greater elevations (38). Damaged muscle fiber structures were pointed out as being the cause for the rise, but one study of repeated eccentric exercise caused almost no increase in CK levels (39). CK levels demonstrate considerable variability influenced by factors such as sex, race, and the type of exercise performed. Notably, eccentric exercise is generally associated with more significant muscle damage compared to concentric contractions of the same intensity. This discrepancy highlights the importance of considering these variables when interpreting CK levels as muscle stress and damage indicators (40). Understanding these differences is essential for accurately assessing muscle response and recovery in diverse populations and exercise modalities (41).
Consequently, delayed onset muscle soreness and associated inflammatory responses are typically observed within this time. Pal et al. (2018) also noted that interval training increases LDH, CK, and liver enzyme levels within 24 to 48 hours following training. Therefore, the timing of assessments after HIIT is critical for evaluating inflammation and muscle damage markers (42). Given that individuals with overweight status often exhibit lower physical fitness levels, it is essential to consider the effects of high-intensity training, particularly HIIT (43). Rohnejad and colleagues investigated the acute effects of HIIT on inflammatory and muscle damage indices in overweight middle-aged men and the kinetics of these markers at 1, 24, and 48 hours post-training (44). Additionally, these markers correlate with frailty, morbidity, and mortality. Notably, CRP levels are lower in individuals who engage in moderate exercise than those who are inactive (32,45).
The majority of studies have reported an increase in IL-10 following intense exercise, aligning with earlier findings (32,46). However, Allen et al. (2017) highlighted that IL-10 production in response to strenuous acute exercise is variable, with some studies reporting increases, others indicating decreases, and some showing no changes, depending on the exercise protocols and analytical methods employed (32). Nonetheless, IL-10 levels typically peak during the recovery phase post-exercise, with the extent of this increase being associated with both the active muscle mass engaged and the intensity of the exercise performed. Recent reviews by Cabral‐Santos et al. (2019) emphasize that the duration of training is the most critical factor influencing the magnitude of the exercise-induced increase in plasma IL-10 levels (47). This elevation in IL-10 may protect against potential chronic low-grade inflammation and tissue damage.
In a competitive tournament setting, goalball athletes may be required to participate in multiple matches within a condensed timeframe. Assessing the concentrations of IL-6, CK, and LDH 48 hours post-training can provide valuable insights into the recovery processes of players between games, as well as the potential impact on their performance in subsequent competitions. Furthermore, an elevation in IL-6, CK, and LDH levels following exercise can indicate muscle damage or fatigue, heightening the risk of injury. By closely monitoring these biomarker concentrations, coaches can effectively identify players who may be predisposed to injury and implement appropriate preventive strategies.
It is essential to consider that the participants in this study are individuals with special needs, and the act of venipuncture can elicit discomfort and sensitivity. Consequently, the optimal approach would involve conducting blood sampling 48 hours after the exercise sessions. Additionally, it is recommended to evaluate biomarker levels immediately post-training and at 6, 12, and 24 hours after that. These considerations are acknowledged as limitations within the scope of the study. One of the limitations of the present study is the lack of control over the psychological conditions of the players. The following limitation was that the current study was conducted on male goalball players aged 21 to 27 years, and the generalization of the results is only possible on similar age and gender groups. Another limitation of this study is the lack of measuring variables immediately, 12 hours, and 24 hours after the exercises. Due to the fact that the test subjects were particular (Blind or severely visually impaired) and were sensitive to blood sampling and invasive methods, we were faced with this limitation. It is better to investigate the effect of such exercises on other age and gender groups in future research due to the limitations of the current research. Moreover, the functional tests of this sport should be evaluated, and their relationship with physiological changes in the players should be investigated and analyzed. Also, by conducting a similar study in different sports and comparing its results with the present study, a practical solution can be provided to improve players' performance, reduce the risk factors of injury, and prevent them.
In summary, the changes in IL-6, CK, and LDH levels observed in the study reflect the physiological responses to different training intensities. While initially causing more significant muscle damage and metabolic stress, HIIT fosters adaptations that improve muscle recovery and integrity, as evidenced by the substantial reductions in CK and LDH levels over the training period. In contrast, MIIT promotes a more stable response with less acute damage, highlighting the importance of training intensity in influencing muscle health and recovery in goalball players.
Conclusion
Our study demonstrated that HIIT and MIIT for eight weeks could improve the concentration of CK, LDH, and IL-6 in goalball players. Moreover, HIIT had more effect than MIIT for eight weeks. Based on our data, performing HIIT and MIIT may consistently increase the capacity of the physiology of goalball players.
Acknowledgement
No acknowledgment.
Funding sources
No funding.
Ethical statement
All procedures have been approved by the ethics committee of Islamic Azad University of Isfahan (Khorasgan) with the number IR.IAU.KHUISF.REC.1402.381 and were carried out according to the Declaration of Helsinki. Before starting the study, informed consent was obtained from all the participants who participated in the study.
Conflicts of interest
The authors declare that they have no conflict of interest.
Author contributions
AM carried out the experiments and drafted the manuscript, FT participated in this study as supervisor and contributed to study design, conceptualization, data analysis and validation, and revising the manuscript. KhJD and ZJ participated in data validation and revising the manuscript. All authors read and approved the final manuscript.
Type of Article: Original article |
Subject:
Health
Received: 2024/04/30 | Accepted: 2024/06/24 | Published: 2024/06/30
Received: 2024/04/30 | Accepted: 2024/06/24 | Published: 2024/06/30
References
1. Cursiol JA, de Arruda TB, Nakamura FY, Barbieri RA. Three simulated goalball games in the same day cause central fatigue and can impair game technical performance. Adapt Phys Activ Q. 2022;39(3):356-73. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Utvić N, Lilić L, Dubey VP, Nikolić M, Aleksandrović M. Effects of application of goalball at classes of physical education on some motoric abilities and physical constitution of school age boys. Homo Sporticus. 2022;24(1):19-24. [View at Publisher] [Google Scholar]
3. Esatbeyoglu F, Ekinci YE, Köse MG, Hazır T, Kin-İşler A, Haegele JA. Longitudinal changes in body composition, physiological characteristics, and motor performance of Paralympic goalball athletes. Br J Vis Impair. 2024:02646196241226835. [View at Publisher] [DOI] [Google Scholar]
4. Alves I, Gomide L, Rocha MJ, Vizu T, Aquino R, Menezes R, et al. Reliability and validity of an observational system to qualify performance indicators in goalball matches: Scal-Go proposal. European Journal of Adapted Physical Activity. 2022;15:1. [View at Publisher] [DOI] [Google Scholar]
5. Coates AM, Joyner MJ, Little JP, Jones AM, Gibala MJ. A perspective on high-intensity interval training for performance and health. Sports Med. 2023;53(Suppl 1):85-96. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Ojo OR. Selected physiological responses to interval training in the enhancement of physical fitness. Sapientia Foundation Journal of Education, Sciences and Gender Studies. 2020;2(3):211-23. [View at Publisher] [Google Scholar]
7. Munro H. An investigation into potential methods of improving the fitness stimulus associated with small-sided games in soccer 2014. [Doctoral dissertation] [View at Publisher] [Google Scholar]
8. Alves IdS, Kalva-Filho CA, Aquino R, Travitzki L, Tosim A, Papoti M, et al. Relationships between aerobic and anaerobic parameters with game technical performance in elite goalball athletes. Front Physiol. 2018;9:1636. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Vanlandewijck YC, Thompson WR. Handbook of sports medicine and science: the Paralympic athlete:John Wiley & Sons;2011. [View at Publisher] [DOI] [Google Scholar]
10. Hadiono M, Kushartanti BW, editors. High intensity interval training (HIIT) and moderate intensity training (MIT) against TNF-α and IL-6 levels in rats. 2nd International Conference on Sports Sciences and Health 2018 (2nd ICSSH 2018):Atlantis Press;2019. [View at Publisher] [DOI] [Google Scholar]
11. Stöggl TL, Björklund G. High intensity interval training leads to greater improvements in acute heart rate recovery and anaerobic power as high volume low intensity training. Front Physiol. 2017;8:562. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Iturricastillo A, Granados C, Cámara J, Reina R, Castillo D, Barrenetxea I, et al. Differences in physiological responses during wheelchair basketball matches according to playing time and competition. Res Q Exerc Sport. 2018;89(4):474-81. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Katagiri H, Forster BB, Koga H, An J-S, Adachi T, Derman W. Noteworthy Performance of Muscle-Injured Para-Athletes: A Study of Magnetic Resonance Imaging-Detected Muscle Injuries at the Tokyo 2020 Summer Paralympic Games. Am J Phys Med Rehabil. 2024;103(7):652-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Sarkar S, Debnath M, Das M, Bandyopadhyay A, Dey SK, Datta G. Effect of high intensity interval training on antioxidant status, inflammatory response and muscle damage indices in endurance team male players. Apunts Sports Medicine. 2021;56(210):100352. [View at Publisher] [DOI] [Google Scholar]
15. Goulart-Siqueira G, Benítez-Flores S, Ferreira AR, Zagatto AM, Foster C, Boullosa D. Relationships between different field test performance measures in elite goalball players. Sports (Basel). 2018;7(1):6. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Gulick DT, Malone LA. Field test for measuring aerobic capacity in Paralympic goalball athletes. International Journal of Athletic Therapy & Training. 2011;16(5):22. [View at Publisher] [DOI] [Google Scholar]
17. Abedpoor N, Taghian F, Ghaedi K, Niktab I, Safaeinejad Z, Rabiee F, et al. PPARγ/Pgc-1α-Fndc5 pathway up-regulation in gastrocnemius and heart muscle of exercised, branched chain amino acid diet fed mice. Nutr Metab (Lond). 2018;15:59. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Li W, Li H, Zheng L, Xia J, Yang X, Men S, et al. Ginsenoside CK improves skeletal muscle insulin resistance by activating DRP1/PINK1-mediated mitophagy. Food Funct. 2023;14(2):1024-36. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Costello JT, Rendell RA, Furber M, Massey HC, Tipton MJ, Young JS, et al. Effects of acute or chronic heat exposure, exercise and dehydration on plasma cortisol, IL-6 and CRP levels in trained males. Cytokine. 2018;110:277-83. [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Barrak MH, Dawood FA, Abed Shubar SN, Al-fahham AA. Pathophysiology, The Biochemical and Clinical Significance of Lactate Dehydrogenase. International Journal of Health and Medical Research. 2024;03(07):440-3. [View at Publisher] [DOI] [Google Scholar]
21. Yao S, Chai H, Tao T, Zhang L, Yang X, Li X, et al. Role of lactate and lactate metabolism in liver diseases. Int J Mol Med. 2024;54(1):59. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Farhana A, Lappin SL. Biochemistry, lactate dehydrogenase. Treasure Island (FL):StatPearls Publishing;2024. [View at Publisher] [PMID] [Google Scholar]
23. Jabbar AH, Abd MAAA-A, Batouli AN. The effect of synchronized training on enzymes (LDH-CPK) and skill performance in football among ages 17-19. International Journal of Physiology, Nutrition and Physical Education. 2023;8(1):309-14. [View at Publisher] [Google Scholar]
24. Abedpoor N, Taghian F, Hajibabaie F. Cross brain-gut analysis highlighted hub genes and LncRNA networks differentially modified during leucine consumption and endurance exercise in mice with depression-like behaviors. Mol Neurobiol. 2022;59(7):4106-23. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Abedpoor N, Taghian F, Jalali Dehkordi K, Safavi K. Sparassis latifolia and exercise training as complementary medicine mitigated the 5-fluorouracil potent side effects in mice with colorectal cancer: bioinformatics approaches, novel monitoring pathological metrics, screening signatures, and innovative management tactic. Cancer Cell Int. 2024;24(1):141. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. Kaviani E, Hajibabaie F, Abedpoor N, Safavi K, Ahmadi Z, Karimy A. System biology analysis to develop diagnostic biomarkers, monitoring pathological indexes, and novel therapeutic approaches for immune targeting based on maggot bioactive compounds and polyphenolic cocktails in mice with gastric cancer. Environ Res. 2023;238(pt 2):117168. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Małkowska P, Sawczuk M. Cytokines as biomarkers for evaluating physical exercise in trained and non-trained individuals: a narrative review. Int J Mol Sci. 2023;24(13):11156. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Nash D, Hughes MG, Butcher L, Aicheler R, Smith P, Cullen T, et al. IL‐6 signaling in acute exercise and chronic training: Potential consequences for health and athletic performance. Scand J Med Sci Sports. 2023;33(1):4-19. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Alkahtani S. Comparing fat oxidation in an exercise test with moderate-intensity interval training. J Sports Sci Med. 2014;13(1):51-8. [View at Publisher] [PMID] [Google Scholar]
30. Leiva-Valderrama JM, Montes-de-Oca-Garcia A, Opazo-Diaz E, Ponce-Gonzalez JG, Molina-Torres G, Velázquez-Díaz D, et al. Effects of high-intensity interval training on inflammatory biomarkers in patients with type 2 diabetes. A systematic review. Int J Environ Res Public Health. 2021;18(23):12644. [View at Publisher] [DOI] [PMID] [Google Scholar]
31. Atakan MM, Li Y, Koşar ŞN, Turnagöl HH, Yan X. Evidence-based effects of high-intensity interval training on exercise capacity and health: A review with historical perspective. Int J Environ Res Public Health. 2021;18(13):7201. [View at Publisher] [DOI] [PMID] [Google Scholar]
32. Allen NG, Higham SM, Mendham AE, Kastelein TE, Larsen PS, Duffield R. The effect of high-intensity aerobic interval training on markers of systemic inflammation in sedentary populations. Eur J Appl Physiol. 2017;117(6):1249-56. [View at Publisher] [DOI] [PMID] [Google Scholar]
33. Costa Santiago DD, Silva Lopes JS, de Magalhães Neto AM, Balbinotti Andrade CM. Analysis of Biomarkers in Response to High Intensity Functional Training (HIFT) and High Intensity Interval Training (HIIT): A Systematic Review Study. Archives of Current Research International. 2021;21(3):59-72. [View at Publisher] [DOI] [Google Scholar]
34. Da Rocha AL, Pereira BC, Teixeira GR, Pinto AP, Frantz FG, Elias LLK, et al. Treadmill slope modulates inflammation, fiber type composition, androgen, and glucocorticoid receptors in the skeletal muscle of overtrained mice. Front Immunol. 2017;8:1378. [View at Publisher] [DOI] [PMID] [Google Scholar]
35. Dorneles GP, Haddad DO, Fagundes VO, Vargas BK, Kloecker A, Romão PR, et al. High intensity interval exercise decreases IL-8 and enhances the immunomodulatory cytokine interleukin-10 in lean and overweight-obese individuals. Cytokine. 2016;77:1-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
36. Pengam M, Goanvec C, Moisan C, Simon B, Albacète G, Féray A, et al. Moderate intensity continuous versus high intensity interval training: Metabolic responses of slow and fast skeletal muscles in rat. Plos One. 2023;18(10):e0292225. [View at Publisher] [DOI] [PMID] [Google Scholar]
37. Burt D, Doma K, Connor J. The effects of exercise-induced muscle damage on varying intensities of endurance running performance: A systematic review and meta-analysis. Science & Sports. 2023;38(7):647-62. [View at Publisher] [DOI] [Google Scholar]
38. Moghadam-Kia S, Oddis CV, Aggarwal R. Approach to asymptomatic creatine kinase elevation. Cleve Clin J Med. 2016;83(1):37. [View at Publisher] [DOI] [PMID] [Google Scholar]
39. Baumert P, Lake MJ, Stewart CE, Drust B, Erskine RM. Genetic variation and exercise-induced muscle damage: implications for athletic performance, injury and ageing. Eur J Appl Physiol. 2016;116(9):1595-625. [View at Publisher] [DOI] [PMID] [Google Scholar]
40. Li G, Li Z, Liu J. Amino acids regulating skeletal muscle metabolism: mechanisms of action, physical training dosage recommendations and adverse effects. Nutr Metab (Lond). 2024;21(1):41. [View at Publisher] [DOI] [PMID] [Google Scholar]
41. Lira FS, Dos Santos T, Caldeira RS, Inoue DS, Panissa VL, Cabral-Santos C, et al. Short-term high-and moderate-intensity training modifies inflammatory and metabolic factors in response to acute exercise. Front Physiol. 2017;8:856. [View at Publisher] [DOI] [PMID] [Google Scholar]
42. Pal S, Chaki B, Chattopadhyay S, Bandyopadhyay A. High-intensity exercise induced oxidative stress and skeletal muscle damage in postpubertal boys and girls: a comparative study. J Strength Cond Res. 2018;32(4):1045-52. [View at Publisher] [DOI] [PMID] [Google Scholar]
43. Calıskan E, Pehlivan A, Erzeybek MS, Kayapınar FC, Agopyan A, Yuksel S, et al. Body mass index and percent body fat in goalball and movement education in male and female children with severe visual impairment. Neurol Psychiatry Brain Res. 2011;17(2):39-41. [View at Publisher] [DOI] [Google Scholar]
44. Rohnejad B, Monazzami AA. Effects of high-intensity intermittent training on some inflammatory and muscle damage indices in overweight middle-aged men. Apunts Sports Medicine. 2023;58(217):100404. [View at Publisher] [DOI] [Google Scholar]
45. Fedewa MV, Hathaway ED, Ward-Ritacco CL. Effect of exercise training on C reactive protein: a systematic review and meta-analysis of randomised and non-randomised controlled trials. Br J Sports Med. 2017;51(8):670-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
46. Moldoveanu AC, Diculescu M, Braticevici CF. Cytokines in inflammatory bowel disease.Rom J Intern Med. 2015;53(2):118-27. [View at Publisher] [DOI] [PMID] [Google Scholar]
47. Cabral‐Santos C, de Lima Junior EA, Fernandes IMdC, Pinto RZ, Rosa‐Neto JC, Bishop NC, et al. Interleukin‐10 responses from acute exercise in healthy subjects: A systematic review.J Cell Physiol. 2019;234(7):9956-65. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
